Chronic UTI in children

Chronic urinary tract infection (UTI) in not confined to adults. The confronting reality that is starting to emerge is that children can, and do, develop chronic UTI. This often leads to immense distress and suffering for the child and considerable stress and anxiety for the family. Chronic UTI in children is far less studied and understood than in adults, and access to effective, curative treatment appears to be difficult, at best.
Common acute UTI symptoms in children
Typical acute UTI symptoms in children are similar to those experienced by adults and can be extremely painful and debilitating. Unmanageable incontinence is very common and can have profound psychological impacts for school aged children. Other painful and distressing UTI symptoms children can experience include:
- Sudden urinary urgency and frequency, daytime and nighttime
- Incontinence, daytime and nighttime (bed wetting)
- Pain, burning, stinging when urinating (dysuria)
- Urinary retention
- Abdominal, loin or lower back pain
- Localised genitourinary pain
- Cloudy or frank blood in urine
- Foul-smelling urine
Nonspecific acute UTI symptoms in infants and children can include:
- Fever
- Lethargy
- Unexplained crying, irritability, fussiness
- Vomiting and diarrhea
- Loss of appetite, poor feeding, refusing to feed.
When to seek urgent medical attention
The Sydney Children’s Hospitals Network website says you should seek urgent medical attention if your child shows signs of a more severe UTI or an infection that has spread, such as:
- fever that does not go down
- back pain
- feeling very tired.
UTI testing and treatment guidelines for children
Various guidelines from different states and jurisdictions are available for acute and recurrent UTI in children.7 8 9 10 11 12 However, the flawed diagnostic recommendations mirror those in adult UTI, with the guidelines supporting the use of insensitive, inaccurate urine culture to diagnose and direct treatment. As with adults, there are currently no nationally consistent, evidence-based guidelines for the diagnosis and management of chronic UTI in children.
Without more research looking specifically at chronic UTI in children, it can only be assumed that, as in adults, existing methods are inept at diagnosing chronic UTI in children, and that treatment failures using the existing guidelines’ recommendations are not uncommon.
What are the symptoms of chronic UTI in children?
According to Australian paediatric urologist and researcher at Sydney’s Westmead Children’s Hospital, Associate Professor Anirudh (Ani) Deshpande, common symptoms indicating suspected chronic UTI in children include:
- Clustering of symptomatic episodes characterised by stinging and burning during passing urine that can be stopped temporarily with antibiotic treatment
- coli growth in multiple urine samples
- Presence of white blood cells (pyuria) in most urine samples, even when feeling well
- Malaise, fatigue, lower abdominal pain
- Urinary leakage.
Dr Deshpande has observed that children with chronic UTI have more than one of these problems.
What to do if you think your child has a chronic UTI
Prepare for your child’s doctor’s appointment
Unfortunately, many doctors are unaware of the current evidence on UTI testing and treatment and may be unfamiliar with the existence of chronic UTI in both adults and children. This means that you need to be proactive, positive, and persistent in advocating for your child.
Top tips for preparing to speak with your child’s doctor
- Keep copies of your child’s UTI test reports.
- Educate yourself on chronic UTI.
- Visit the ‘Do I have a chronic UTI?’ page on our website for more information about preparing for an appointment with your doctor to discuss chronic UTI. This page is written for adults but can also be applied to your child.
The Better Health Channel also shares useful tips on how to prepare for an appointment with your doctor.
Consider joining our ‘Suspected chronic UTI in children’ register
Currently, there is an almost total lack of information about chronic UTI in children, and limited avenues for parents to receive new information that may help their own and others’ children.
Chronic UTI Australia has set up a register to collect basic information about children who have a diagnosis of chronic UTI, or whose parents suspect they have a chronic UTI. This will allow us to keep a record of your details and to get in touch with you if we have new information to share.
Any information you provide to the register will be treated in strict confidence and would not be shared outside our organisation without your written permission. The preamble to the register provides details of our privacy policy.
The register can be accessed here:
Research into paediatric chronic UTI
Research into UTI, especially in children, is grossly underfunded world-wide. The consequence is that advancements in diagnostic and treatment protocols are extremely slow. This means medical practitioners are left to rely on guidelines that were developed based on scientific evidence that is now understood to be outdated, and potentially harmful in some instances.
Australian research
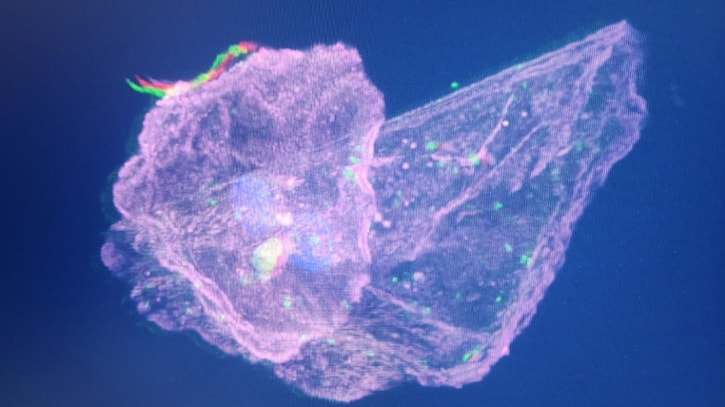
A confocal micrograph showing bacterial colonisation of a urothelial cell taken from a child. Micrograph courtesy of Associate Professor Anirudh Deshpande, Sydney, Australia
Recently, Associate Professor Aniruddh (Ani) Deshpande, an Australian paediatric urologist, discovered that bacteria had colonised epithelial cells (the cells that line the bladder) in a 10-year-old patient who had suffered severe ‘recurrent UTI’ for six years. The child had received numerous standard antibiotic courses to treat repeat infections that presented as acute episodes. She returned both positive and negative urine culture tests during this period. After becoming aware of the potential for infections to become embedded in the urinary tract (chronic UTI), Assoc Prof Deshpande and his research team at the Children’s Hospital at Westmead (Sydney) have since identified bacterial colonisation of bladder wall cells in a high proportion of his paediatric patients (mostly female) who have had multiple UTIs and have a clinical course suspicious of a chronic UTI.13 The tests deployed in these cases are used for research and are intricate, expensive and not readily available.
The research findings in children appear to be strikingly similar to the large body of global research demonstrating intracellular bacterial colonisation in bladders of symptomatic adults.14 15 16 17 18 19 20 21 22 23 24 25 It is becoming increasingly evident that awareness of chronic UTI in children, and treatment protocols for UTI in children, need to drastically change to reflect the current science and address the root cause of infection in this long-suffering patient group.
“Chronic UTI in children which I currently define as self-sustaining, symptomatic intracellular UTI, is an enigma that needs to be studies, explored, exposed and deciphered. We have made a brave start here in Sydney and much more needs to be done. We need to clarify the diagnostic tests that are appropriate and of course, treatments that are safe and effective in children. The treatments may or may not look like what we expect them to be.”
(Dr Ani Deshpande, Sydney, Australia, 2024) Email: dr.ani.deshpande@gmail.com
American research
The Spencer Lab at the Nationwide Children’s Hospital in Columbus, Ohio, USA, study UTI in children. The team, led by Jon David Spencer, is focused on the role of the innate immune system and antimicrobial peptides in regulating and preventing UTI. The team has demonstrated that peptides in the Ribonuclease A Superfamily are important in protecting the urinary tract from invading uropathogens. By studying how peptides prevent UTI, there is potential to develop new non-antibiotic therapies for UTI.
Email: SpencerLab@NationwideChildrens.org
The importance of paediatric chronic UTI research
Although there appear to be strong similarities between chronic UTI in children and adults, at this stage it is unknown if it is the same disease entity. Studying chronic UTI in children may provide a unique opportunity to advance the understanding of chronic UTI in an ‘uncontaminated’ physiology that is not complicated through hormonal changes and sexual activity.
UK advocacy for chronic UTI in children
The Chronic Urinary Tract Infection Campaign (CUTIC) is a patient advocacy organisation established in the United Kingdom in 2016. Following a ban in the UK in 2016 that prevents treatment of chronic UTI in children (under 16 years of age) outside guidelines designed for acute and recurrent UTI,26 the group has been campaigning to reinstate access to appropriate antibiotic treatment for children suffering chronic UTI. We share a selection of articles published by UK news outlets below.
News articles
- https://www.dailymail.co.uk/health/article-12526485/Children-risk-deadly-sepsis-GPs-fail-treat-common-bladder-infections-affecting-one-ten-girls.html
- https://inews.co.uk/news/chronic-uti-children-lack-treatments-homeschooling-2610622
- https://www.itv.com/news/2023-09-14/why-wont-they-help-me-how-a-lack-of-uti-treatment-is-failing-children
- https://inews.co.uk/news/chronic-uti-children-cycles-infection-nice-guidelines-testing-failures-1801998
- https://inews.co.uk/news/health/chronic-uti-life-changing-infection-pain-every-day-1548112
- https://inews.co.uk/news/health/chronic-uti-life-changing-infection-pain-every-day-1548112
- https://www.theguardian.com/society/2019/feb/20/in-pain-all-the-time-will-there-ever-be-relief-for-women-with-chronic-life-changing-utis?fbclid=IwAR0w6KQg8mfqrGj_D3WgldLUyVy27aNI751BuTHbDqPvw8-QvQzxYHxS-eI
Extract from ‘Cystitis Unmasked’
We share a deeply disturbing extract from James Malone-Lee’s book, Cystitis Unmasked (2021). It is written by a young woman in the UK who recounts her personal trauma of chronic UTI in childhood and how her suffering continued until she was legally able to access appropriate treatment as an adult.
A young adult writes of her experiences as a child:
“I developed a chronic UTI as a result of recurrent childhood urinary infections which were repeatedly misdiagnosed and left untreated, resulting in severe bladder and kidney symptoms which left me with a diagnosis of interstitial cystitis. I am now 22 years old and this condition has stripped me of my entire childhood.
“I started to develop symptoms of severe urinary frequency and urgency when I was 6 years old. When my parents initially took me to see my GP, a urine dipstick was carried out and showed no signs of infection. A subsequent culture showed insignificant bacterial growth, resulting in no further treatment. When my symptoms subsequently worsened over the next 3 months, further negative dipsticks and cultures were carried out and I was misdiagnosed with overactive bladder syndrome. By this time, my urinary frequency had progressed to the point where I was urinating every 10 minutes and could not be away from a toilet for any length of time. My parents and school teachers were advised to encourage me to train my bladder to hold more urine by withholding access to a toilet, which resulted in such severe pain and embarrassment that I became terrified of going to school and missed a significant amount of my primary school education.
“Coincidentally, recurrent ear infections throughout my childhood meant that I was prescribed numerous short courses of antibiotics, which somewhat helped to reduce my bladder symptoms. However, my symptoms would recur quickly after the antibiotic course was finished. Despite this clear correlation in symptoms, any suggestion of an infection was dismissed repeatedly by my GP.
“I battled through my teenage years with fluctuating bladder symptoms that often left me leaving the classroom several times during school lessons and avoiding school trips and social interaction for fear of suffering bladder symptoms. When I was 17, I suddenly developed a severe worsening of symptoms, resulting in immense burning during urination, severe urgency, severe bladder pain and a sensation that I had a boiling hot marble stuck in my urethra. I saw my GP, who diagnosed me with a UTI based on my symptoms and prescribed me with a week-long course of antibiotics. However, despite a slight improvement in my symptoms during this time, the symptoms continued to linger. When my GP subsequently sent my urine off for culture, it revealed mixed growth of doubtful significance, and I was diagnosed with “post-UTI irritation” and placed on oxybutynin. This pattern of events continued to repeat over the next 3 months, with numerous short 3-day courses of antibiotics, oxybutynin, Vesicare and amitriptyline being prescribed in an attempt to relieve my pain.
“Over the course of the next 2 years, my symptoms continued to worsen. I saw my GP hundreds of times and was referred to a total of two urogynaecologists and two urologists, all of whom either diagnosed me with overactive bladder or interstitial cystitis, and one of who claimed that my symptoms were psychological in nature and that my brain was simply “wired differently” to everyone else. I underwent two urodynamic studies, three KUB ultrasounds and two rigid cystoscopies under anaesthetic, the second of which I also underwent a ureteroscopy, retrograde study, urethral dilation, ureter dilation and bladder distension following a misdiagnosis of kidney stones after a poor-quality CT scan. Unfortunately, these investigations caused a massive deterioration in my symptoms and I was hospitalised on multiple occasions with severe uncontrollable pain and vomiting, kidney infections, urinary retention and passing frank blood clots that were so thick that I was unable to pass urine. Each time I was admitted to hospital and given IV antibiotics, my symptoms would improve dramatically, only to relapse as soon as the course had finished.
“By the time I self-referred to ***** private clinic in 2015, I was near suicidal with pain. My symptoms included severe, debilitating pain in my urethra, bladder, kidneys and vagina, urine retention that frequently left me unable to pass urine for 24 hours at a time, significant voiding issues and incredible urgency which felt as though my bladder was tying itself in knots. I frequently passed thick blood clots, and the immense urethral burning that plagued me with this condition felt as though someone had filled my urethra with petrol and set it on fire. I often awoke at night screaming with pain because the pain of leaking urine in my sleep was so terrifying that I often thought I was being attacked.
“[The clinic] diagnosed me with a chronic UTI via microscopy on a fresh, unspun urine sample and immediately placed me on an extended course of antibiotics. Although my progress has been slow as a result of so many years of inadequate treatment resulting in a deeply embedded infection, I have finally reached the stage where my symptoms are under control and I do not require the care of urologists or my GP with regards to my bladder symptoms. I am now able to live a relatively normal life with minimal bladder symptoms, and I have returned to work and university. However, as a result of the extensive strain that my untreated chronic UTI has placed on my autonomic nervous system over the past 16 years, I have been diagnosed with postural orthostatic tachycardia syndrome, inappropriate sinus tachycardia and gastrointestinal motility problems, thought to be due to gastroparesis, which are likely to be ongoing issues throughout my life.
“My greatest regret is that so many opportunities were missed to treat my symptoms when I was a child. Had I been given early access to treatment, my lifelong suffering could have been entirely preventable. I can only hope that in the future, children like myself will not be confined to the suffering and trauma that I have experienced.” 27
Useful articles to read
- https://www.chronicutiaustralia.org.au/chronic-uti/what-is-chronic-uti/
- https://www.chronicutiaustralia.org.au/uti-testing/
- https://www.chronicutiaustralia.org.au/chronic-uti/how-chronic-uti-forms/
- https://www.chronicutiaustralia.org.au/treatment/
References
- https://www.ncbi.nlm.nih.gov/pmc/articles/PMC9865477/
- https://journals.lww.com/pidj/abstract/2008/04000/prevalence_of_urinary_tract_infection_in.4.aspx
- https://www.thelancet.com/journals/lancet/article/PIIS0140-6736(20)30676-0/abstract
- https://www.ncbi.nlm.nih.gov/pmc/articles/PMC10828737/
- https://www.ncbi.nlm.nih.gov/pmc/articles/PMC2907613/
- https://www.ncbi.nlm.nih.gov/pmc/articles/PMC2907613/
- https://www.rch.org.au/clinicalguide/guideline_index/Urinary_tract_infection/
- https://www.sahealth.sa.gov.au/wps/wcm/connect/ebd4e56e-7ae1-408d-b3b1-20c75f9f12de/Urinary+Tract+Infection+in+Children_Paed_v1_0.pdf?MOD=AJPERES&CACHEID=ROOTWORKSPACE-ebd4e56e-7ae1-408d-b3b1-20c75f9f12de-oc-W96p
- https://www.childrens.health.qld.gov.au/for-health-professionals/queensland-paediatric-emergency-care-qpec/queensland-paediatric-clinical-guidelines/urinary-tract-infection
- https://pch.health.wa.gov.au/For-health-professionals/Emergency-Department-Guidelines/Urinary-tract-infection
- https://www.schn.health.nsw.gov.au/urinary-tract-infection-uti-factsheet
- https://www.racgp.org.au/afp/2016/august/paediatric-urinary-tract-infections-diagnosis-and
- https://www.chronicutiaustralia.org.au/wp-content/uploads/2024/04/The-Weekend-Australian.3Feb2024.pdf
- https://www.ncbi.nlm.nih.gov/pmc/articles/PMC3697662/
- https://www.chronicutiaustralia.org.au/chronic-uti/how-chronic-uti-forms/
- https://www.ncbi.nlm.nih.gov/pmc/articles/PMC3868479/
- https://www.ncbi.nlm.nih.gov/pmc/articles/PMC4617679/
- https://www.ncbi.nlm.nih.gov/pmc/articles/PMC1750882/
- https://www.science.org/doi/10.1126/sciadv.adi9834
- https://pubmed.ncbi.nlm.nih.gov/31455657/
- https://www.ncbi.nlm.nih.gov/pmc/articles/PMC4457377/
- https://www.ics.org/Abstracts/Publish/180/000123.pdf
- https://pubmed.ncbi.nlm.nih.gov/18092884/
- https://academic.oup.com/femspd/article/doi/10.1093/femspd/ftae012/7681980?login=false
- https://www.ncbi.nlm.nih.gov/pmc/articles/PMC6801050/
- https://www.theguardian.com/society/2019/feb/20/in-pain-all-the-time-will-there-ever-be-relief-for-women-with-chronic-life-changing-utis?fbclid=IwAR0w6KQg8mfqrGj_D3WgldLUyVy27aNI751BuTHbDqPvw8-QvQzxYHxS-eI
- Malone-Lee, J., Cystitis Unmasked, 2021, pp241-244, tfm Publishing Limited, Castle Hill Barns, Harley, Shrewsbury, UK https://www.tfmpublishing.com/cystitis-unmasked